
⭐ The Different Types of Pain — And Which Treatments Actually Fit Each One
Key Takeaways
Introduction — What 13 Years Outside the System Taught MeThirteen years ago, I entered the pain industry from the outside.I wasn’t a doctor.I wasn’t a...
Introduction — What 13 Years Outside the System Taught Me
Thirteen years ago, I entered the pain industry from the outside.
I wasn’t a doctor.
I wasn’t a physio.
I wasn’t a chiropractor or a TCM physician.
I inherited a family pain clinic and ended up observing thousands of cases across multiple disciplines.
That unusual vantage point revealed an uncomfortable truth that very few practitioners ever see:
The same scan can produce three completely different pain experiences — and each one needs a completely different treatment.
Just recently:
Three patients walked in with nearly identical L5–S1 herniations.
One needed surgery to decompress a severely irritated nerve root.
One recovered with physiotherapy and load management.
One improved most when we calmed deep-tissue inflammation using herbal medicine and restored his confidence in movement — his MRI barely changed, yet his pain dropped dramatically.
Same disc problem.
Different mechanisms.
Different solutions.
This is the part no one explains — not on Google, not in most clinics, and certainly not in the viral videos promising miracle fixes.
Today’s article is the framework that took me more than a decade to understand.
⭐ The Three Types of Pain (Explained in the Real World)
Most people assume all pain is the same.
Science — and real-world outcomes — disagree.
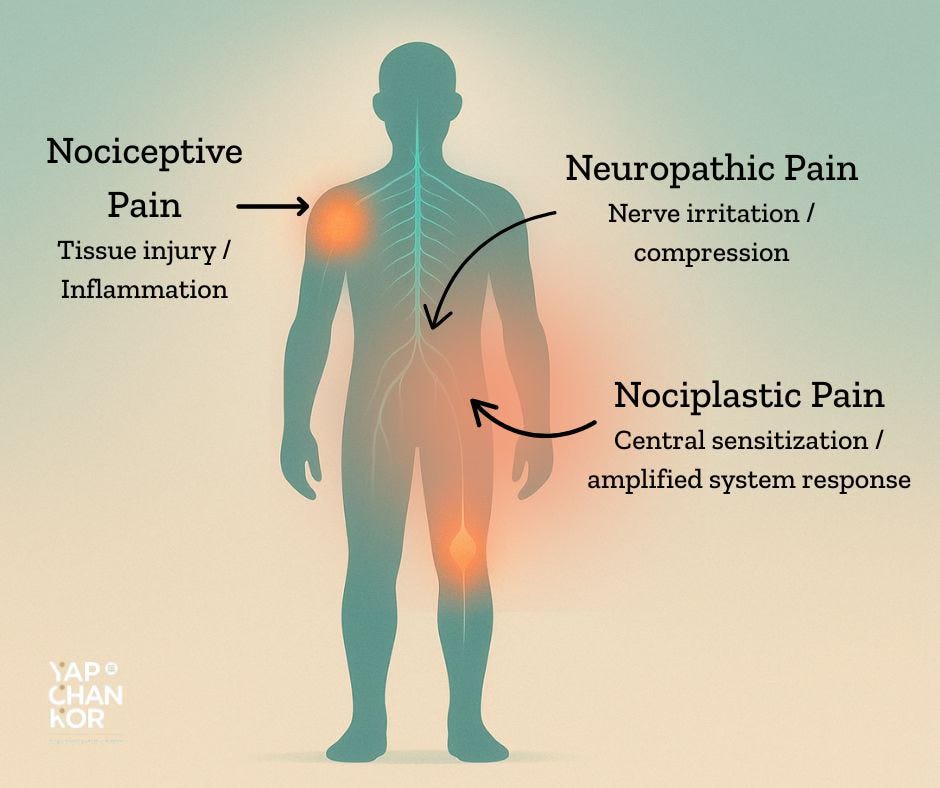
Modern pain research recognises three primary mechanisms the body uses to generate pain.
Think of them as three “languages” your body uses to express distress.
And crucially:
Each type involves several biological systems at once.
Pain is rarely one-dimensional — which is why single treatments often fail.
Below is how we explain them to patients in our clinic, using illustrative examples based on common patterns we see.
1. Nociceptive Pain — When Something in the Body Is Actually Irritated
This is classic injury pain: tissue overload, inflammation, mechanical stress.
Common examples:
sprains, strains, tendon irritation, arthritis flares, disc bulges without nerve symptoms
How it behaves:
predictable, worse with loading, better with rest, responds to anti-inflammatories
An illustrative case
A construction worker developed sharp shoulder pain lifting his arm sideways. He had seen multiple practitioners — massage, adjustments, etc. — all focused on “the shoulder.”
But when we tested his overhead movement under controlled load, the irritated pattern became obvious.
Once we reduced deep-tissue inflammation using our herbal medicine, restored mobility, and strengthened the specific movement he struggled with, his pain improved steadily.
That’s nociceptive pain — mechanical, understandable, treatable when you target the actual tissue stress pattern.
2. Neuropathic Pain — When the Nerve Is Irritated or Compressed
Neuropathic pain is electrical, sharp, burning, or shooting — often unpredictable.
Common causes:
sciatica, nerve entrapment, post-surgical irritation
How it behaves:
burning, tingling, numbness; follows a nerve line; worsens with specific positions
An illustrative case
A man in his 40s had shooting pain down his leg. Massage, cupping, and chiropractic adjustments didn’t help — some made it worse.
The key: his symptoms followed a nerve pathway and eased immediately in decompressed positions.
We focused on nerve-calming strategies:
herbal medicine to reduce deep inflammation
decompression positions
gentle mobility
gradual strengthening
As the nerve settled, the burning and weakness faded.
That’s neuropathic pain — a nerve problem, not a muscle or alignment problem.
3. Nociplastic Pain — When the Nervous System Turns Up the Volume
This is the most misunderstood type of pain.
Nothing is structurally “wrong” in a way a scan can easily show.
The nervous system becomes hypersensitive, treating normal signals as threat.
Common in:
chronic back pain, post-injury lingering pain, widespread pain, poor sleep/stress states
How it behaves:
moving pain, flare-ups, pain out of proportion with scan findings
An illustrative case
A woman in her late 30s had pain that shifted between her hip, back, and ribs. Her MRI was normal. Deep pressure treatments worsened her symptoms.
This was nociplastic pain — a nervous system on high alert.
We changed the approach:
gentle, successful movements
gradual exposure
sleep and stress repair
herbal applications to calm tension without aggressive input
As her system settled, flare-ups reduced significantly.
That’s nociplastic pain — more about the system than the tissue.
⭐ The Hidden Truth: Most People Have More Than One Type at Once
This is where most treatment mismatches happen.
Most real-world pain is a combination of mechanisms.
Examples:
disc bulge → nociceptive + neuropathic
frozen shoulder → inflammatory + mechanical stiffness + sensitisation
knee OA → nociceptive + nociplastic
This is why:
short-term relief fades
treatments “stop working”
you get contradictory advice
Because:
The treatment wasn’t wrong — the mechanism was misidentified.
⭐ ⚠️ FREE ARTICLE ENDS HERE — Continue Reading as a Paid Subscriber
Below this line is where the article becomes practical, actionable, and directly useful for readers trying to understand their own pain.
This is also where the value sharply increases — which is why Substack’s best writers place their paywall here.
🔒 [PAID SUBSCRIBERS] How to Match the Treatment to the Mechanism
(And avoid months or years of trial-and-error)